 As I have written elsewhere on this blog, cardio-respiratory fitness (V02Max) and muscle strength are both independent and powerful predictors of longevity. Ruiz and colleagues carried out the most comprehensive study examining the influence of muscle strength and cardiorespiratory fitness on healthy aging. They found that for those over 60, both all-cause and cancer mortality is twice as likely in individuals with low compared to high skeletal muscle strength, and irrespective of strength, low cardio-respiratory fitness is associated with twice the incidence of all cause mortality. Aging is characterized by a decline in the capacity of the body’s major organs, in particular the loss of muscle (sarcopenia) and loss of bone (osteopenia) have severe consequences on the quality of life as we age. From a metabolic perspective, a healthy muscle mass with frequent exercise provides a sink for glucose, making it easier to maintain blood sugars and avoid insulin resistance. The decline of healthy, functional, skeletal muscle, correspondingly is one of the major factors leading to insulin resistance, with higher levels of insulin causing inappropriate fat deposition throughout the body further compromising organ function. Quite separate from the metabolic effects of diminished muscle mass, the loss of functional endurance, strength and range of motion effects locomotory function, compromises balance, increases risk of falls and fractures and leads to diminished health span. Given the clear benefits of muscle strength on healthy aging one key question is what should you do to preserve muscle mass, strength and function across lifespan? There is clear evidence that the trajectory of sarcopenia and muscle loss is highly dependant on activity - in other words exercise dramatically diminishes the loss of muscle associated with age. Repeated resistance exercise results in increased muscle mass by stimulating protein synthesis within the muscle. With aging there is evidence that there is some anabolic resistance to the effect of exercise but that this can be overcome if a sufficient stimulus is maintained. Protein is the essential macronutrient in the diet for the maintenance of muscle strength, mass and function. The current RDA for protein intake to meet whole-body metabolic demands has been stet at 0.8g/kg/day - but this guideline does not differentiate between young and old or between individuals looking to gain or maintain muscle mass. As with many things nutrition related, these one-size fits all metrics don’t make much sense. A better way to think about protein intake, is that they should be optimized to levels that promote maintenance of muscle mass throughout the lifespan. An interesting recent review looked much more closely at this question of how much protein is optimal if you are trying to gain muscle. This meta analysis found that weight lifting regardless of protein supplementation led to strength gains, but for those who increased their protein strength was increased by about 10% and muscle mass by about 25%. When looking for the optimal amount of protein, the sweet spot seems to be around 1.6 mg/kg/day - or roughly twice the RDA. Above this level there was no additional advantage. Interestingly this review did not find any advantage to the type or timing of the protein intake. This may be because the underlying studies were very small, as there is basic science support for the notion that the muscle’s anabolic response to amino acids is maximal in the post workout period and that branded chain amino acids (BCAA’s), in particular leucine are the most potent stimulators of anabolism through the mTOR pathway. Here's the bottom line:
While I won’t get in too much detail here, I would like to point out that when it comes to macronutrient levels there is no simple formula that fits everyone - in fact this is something that needs to be adjusted to each person’s unique genetics, environment and behaviours. For proteins, we have just seen that the optimal level of protein needs to be adjusted to the level of anabolism - more muscle mass increase requires more protein, maintenance less, and under no circumstances do we want the dietary intake of protein to trigger catabolism or muscle breakdown. So we need to define protein intake by the person’s goals - maintenance or anabolism - and adjust accordingly. Dietary proteins that are not used for the body’s protein repair, maintenance and increase of muscle mass, are generally excreted and not used for energy provision. In many ways, our protein rule is to find the minimum level of protein that meets our goals - maintenance or anabolism. For carbs the task is reversed, we should titrate the maximal amount of carbs that we can tolerate while maintaining low and flat blood sugars without any sign of insulin resistance. For people that are already showing insulin resistance, this level will be very low - hence the low carb approach for metabolic disease. For others, (healthy cross-fitters for example), burning lots of calories in metabolically healthy muscles the amount will be higher. And that brings us to fat, the calories that we do not get from carbs to meet our daily requirements must come from fat. Our energy requirements must be met by our intake of fats and carbs. So it you have insulin resistance and are carb intolerant, your fat intake must increase. For today, I will leave it here, but add one last comment, the most important thing to remember about anything related to nutrition is that the source of any of your calories should be coming from nutrient dense whole foods that are not processed or refined. Humans need to eat. Cells throughout the body are predominantly fueled by glucose delivered through the blood. In evolutionary times food was not predictable, most often scarce, sometimes abundant. To maintain a consistent energy supply of blood glucose, evolution created a complex signaling system to control the process, delivering glucose when it is needed and efficiently storing it, when calories are abundant, ready to be mobilized in times of scarcity. Two hormones are central to this signaling process: insulin and glucagon. When blood sugar drops, pancreatic alpha cells release glucagon which then triggers the release of glucose from the liver. Correspondingly, when blood sugars rise, pancreatic beta cells release insulin which promotes glucose uptake in the liver and muscle, storing it as glycogen initially and then when glycogen stores are maximized, insulin prompts the conversion of carbohydrates and proteins to fat, our most efficient way to store calories for the future. Both insulin and glucagon are small proteins recognized by specific receptors on individual cells. This process, developed over 600M years of evolution, now is under challenge in humans. The conditions for which we are optimized: calorie scarcity with intermittent abundance, no longer exist. Instead we live in a world of continuous excess calories, with processed foods that rapidly spike blood sugars and trigger massive insulin release, and correspondingly massive insulin directed storage of excess calories as fat in adipose tissue. For many this process has become a one-way street, the flexibility to shift metabolically from glucose to fat as fuel that was once the key to our survival has, for many people, been lost. They are dependent on maintaining blood sugars through the constant consumption of carbohydrates. - if you find yourself craving sweats, getting tired after eating and feeling generally fatigued - this could be happening to you.  As a result of excess calories, sedentary lifestyles and this loss of metabolic flexibility, global levels of obesity are soaring: 2 Billion people are overweight - 650M are obese. In Canada close to 50% of the population is overweight!. With obesity has come a corresponding epidemic of obesity related diseases:
The cellular mechanisms by which insulin resistance manifests are complex and beyond the scope of this blog, but at a high level, dysfunctions in three areas appear to alone, or in combination affect the ability of insulin to efficiently activate the insulin receptor and trigger the cascade of reactions that allows insulin to do it's job:
The process by which insulin resistance progresses to pre-diabetes and diabetes is understandable and predictable - it is also very preventable. As insulin resistance sets in, muscle, fat, and liver cells do not respond properly to insulin and thus cannot easily absorb glucose from the bloodstream. As a result, the body needs higher levels of insulin to help glucose enter cells. The beta cells in the pancreas try to keep up with this increased demand for insulin by producing more. As long as the beta cells are able to produce enough insulin to overcome the insulin resistance, blood glucose levels stay in the normal range. Over time, the processes that led to insulin resistance in the first place cause pancreatic beta cells to become less efficient and eventually triggers beta cell death. As this begins to happen, blood sugars fall out of the normal range and people begin to be diagnosed with pre-diabetes or diabetes on the basis of abnormal blood sugars. The time that it takes to progress from insulin resistance to pre-diabetes is generally in the order of 10-15 years - during this whole time a person will have normal blood sugars and may feel reassured that they do not have diabetes - YET - they are manifesting the underlying process of insulin resistance that will lead to diabetes and it's complications. So the big question that you should be asking is - how do I know whether I have insulin resistance? Direct testing of insulin response is not broadly available, so we are most often left looking for other signs of insulin resistance. For the most part, we can work with this:
My blood sugars are normal, but I think I have insulin resistance, what do I do The good news is the process that leads to diabetes is reversible through lifestyle changes:
One of the major reasons we started Wellness Garage was to help people intervene early in preventable disease processes like insulin resistance rather than wait until blood sugars become abnormal (after 10-15 years!) and prescribe medications. If you think that you could be affected by insulin resistance - please reach out to us and book a free consultation, we can help you come up with a plan to address your health needs. 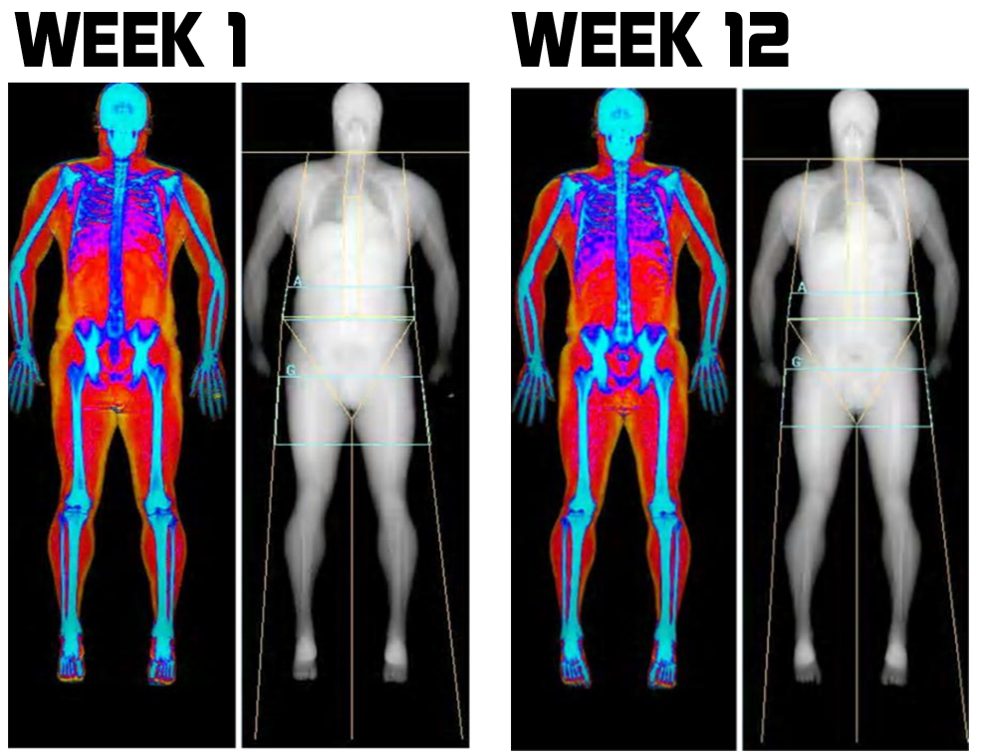 Dual X-ray Absorptiometry - DXA is the Gold Standard for body composition. The technology uses two x-ray beams of differing energy levels to scan a person’s whole body. The difference in the absorption of the two beams by the three major body compartments: bone mass, lean muscle and fat provides the data that allows for a computer to determine a person’s:
Modern lifestyle, with too much food (of questionable quality) and too little exercise leads to some inevitable consequences. Body fat increases, lean muscle mass decreases and bone density decreases. From a physiological perspective, there is nothing inherently wrong here - this is actually how the body was designed:
Most often these changes are recognized when a person becomes overweight and we use their Body Mass Index (BMI) - an index that attempts to define the amount of tissue per standardized unit of height - it does this simply by dividing the height by the weight squared and is measured in kg/m2. But BMI does not differentiate between bone, muscle or fat. So if you are very strong with large muscles and large bones on an average or even small frame - your BMI may tell you that you are overweight. Commonly accepted BMI ranges are underweight: under 18.5 kg/m2, normal weight: 18.5 to 25, overweight: 25 to 30, obese: over 30. More challenging then the strong muscular person who is labelled overweight (most physicians generally recognize this), is the opposite situation: a person with decreased lean muscle, decreased bone density and increased fat where their BMI places them as normal even though from a body fat percentage they are obese. This is far harder to detect in clinical practice, and is probably more common than most realize. The second reason to want a DXA - even if, in fact, especially if, you are obese, is to understand the nature of your obesity. Fat accumulation around the visceral organs in the abdomen is highly associated a destructive self reinforcing cycle of inflammation, insulin resistance, high blood sugars, hypertension, hypercholesterolemia and in turn more adipose fat accumulation. This viscous cycle, known as metabolic syndrome, is highly associated with diabetes, heart disease and stroke. Shockingly, according to a 2011 study almost 1 in 5 (19.1%) of Canadians are estimated to have metabolic syndrome, and most are undiagnosed, (and I suspect things have gotten worse in the last 7years!) The most common component of metabolic syndrome in Canadians: abdominal obesity. A low tech approach to estimating abdominal obesity is to measure the waist to hip ratio - anything above 0.9 for men and 0.85 for women is considered by the WHO to signify abdominal obesity. Less accurate than a DXA and without the lean muscle and bone density information, but a critical metric nonetheless. 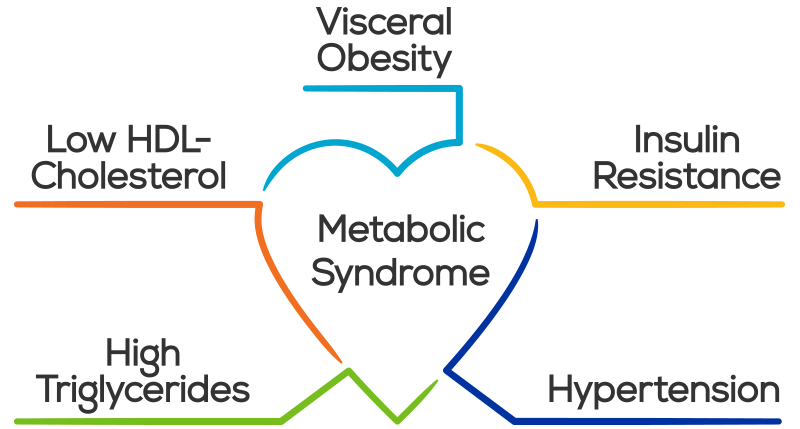 Reason #3 - DXA provides hard-to-get-otherwise information
Maintaining lean muscle mass, along with strength and bone density are strongly positive indicators for longevity - or said another way: loss of muscle mass and bone density are associated with premature death. Here the challenge for the clinician is greater than with abdominal obesity. Often there is simply no way to know a patients lean muscle mass and bone density without DXA measurement. Reason #4 - this is the best part So we now know that DXA gives us some really good information, but the best part is that all of the important markers for vital longevity it tracks
Reason #5 - DXA scans are very safe and can be repeated multiple times in a year. But don’t they use x-ray radiation?
Reason #6 - DXA scans are relatively inexpensive DXA for total body composition is not an insured service, so cost will be an issue for some. However, given the nature of the test and the data they produce for many DXA's are a cost effective investment in their health. ($120 for the first test; $100 for follow-up scans.) In summary - 6 Reasons Why DXA Scans are so useful
At Wellness Garage, we are proud to announce that Bodycomp Imaging is locating a DXA scan within our facility that will be available for our clients as part of our assessments. We are very excited to see this technology come to the South Surrey/White Rock area. Clients are free to book with Wellness Garage or Bodycomp at their convenience. * Wellness Garage and Bodycomp are independent businesses - and Wellness Garage derives no profit from DXA scans done at our facility. |
AuthorDr. Brendan Byrne Categories
All
|
 RSS Feed
RSS Feed