|
For many physicians of my era (started practice in 1991) the story of hormone replacement therapy reflects the bandwagon nature of medicine. In the mid-nineties as I opened my practice, we actively recommended that almost all menopausal women should take hormone replacement (HRT) or estrogen replacement therapy (if they had a hysterectomy). As physicians we measured ourselves by our HRT percentage - feeling that if we were doing our jobs this should approach 100%.  The reasons for our enthusiasm for estrogen replacement seemed clear. In menopause, estrogen levels plummet to 1% of pre-menopausal levels. Using estrogen to replace this loss, appeared to have significant benefits:
...and while these benefits were offset by a small but real increased risk in venous blood clots - the benefits seemed overwhelming. Then on July 17, 2002 the world of estrogen replacement came crashing down. The Woman's Health Initiative - the largest and most expensive trial ($1B) ever done at that time was stopped because HRT increased the risk of breast cancer by 26%. Overnight, physicians jumped off the bandwagon and rates of HRT fell dramatically. Unfortunately most of us did not read the details of the study (once it was eventually released).  In the new book, "Estrogen Matters" by Dr. Avrum Bluming and Carol Tavris, the data from WHI is examined in the broader context.
Starting with the conclusion that HRT increases breast cancer by 26% - the first and most stunningly underappreciated fact was that this increase did not meet statistical significance, meaning that it did not clear the commonly accepted threshold that there has to be less than a 5% chance that this result could be random. Next, even if you accepted that the result was real and not random, then it is important to understand the result. There are two ways that the study could have shown an increased rate of breast CA, either the rate of breast CA actually increased in the treatment group OR the rate of breast CA went down in the control group. Of course if the latter explanation is correct then the study is flawed. Closer analysis of the WHI data has clearly shown that the reported increase rate of breast CA did not come from higher breast cancer rates than expected in the treatment group but resulted from the fact that the control group had a lower incidence of breast cancer than expected. Even more confusing was the fact that this reduction of breast cancer in the control group occurred because there was a significant number of woman who had been on HRT previously and in this group there was less breast cancer. So the WHI concluded that HRT increases breast CA because previous HRT experience decreased the rate of breast CA in the control group - incredible! The third thing to consider when reviewing the WHI findings is the absolute rate of the increase in breast cancer. So even if you accept that the effect is real and not the result of randomness or a decreased rate in the control group the absolute increase in was 8 more breast cancer diagnoses per 10,000 patient years. Taken together, this review significantly decreases, if not removes altogether, the concern that I have about estrogen causing an increase in breast cancer. Bluming and Tavris then revisit the benefits and risks of HRT - providing links to the best available current evidence and in doing so provide perhaps the best single source of HRT information for anyone considering HRT. Summary of the Risks and Benefits of Estrogen Replacement: Benefits
Risks
Bottom Line: For every woman going through menopause, HRT should be given personalized and individualized consideration. I highly recommend this book to anyone who wants to review the data for themselves and make a fully informed decision. As for my physician colleagues, I have already been recommending "Estrogen Matters" For a great listen - check out Peter Attia's podcast. with Bluming and Tavris You may be interested: Osteoporosis Considering the Role of Estrogen Therapy Osteoporosis The Science of Bone Health - 3 Principles to Develop and Maintain Bone In our third bone health post we are going to look specifically at the medical approaches to supplement our lifestyle approach. Our conclusions will not change: The best osteoporosis strategy is to do everything to avoid the likelihood of falling, while providing the best lifestyle support to decrease the rate of bone loss. When it comes to osteoporosis, the strategy must be to decrease the consequences:
It is important to remember that there are more fractures in people who do not have osteoporosis than in people that do; again reiterating the point that preventing the falls that cause the fractures is the most important thing you can do to decrease risk. For woman at risk for osteoporosis, there is an additional strategy that must be considered - estrogen. The key risk factors for osteoporosis are:
For maintaining bone mass there is no other therapy as effective as estrogen replacement starting early in menopause. For both women and men - peak bone mass is achieved in early adulthood, and through an active lifestyle, with adequate nutrition (calcium and protein), and Vitamin D, maintained until middle age when it begins to drop more rapidly. 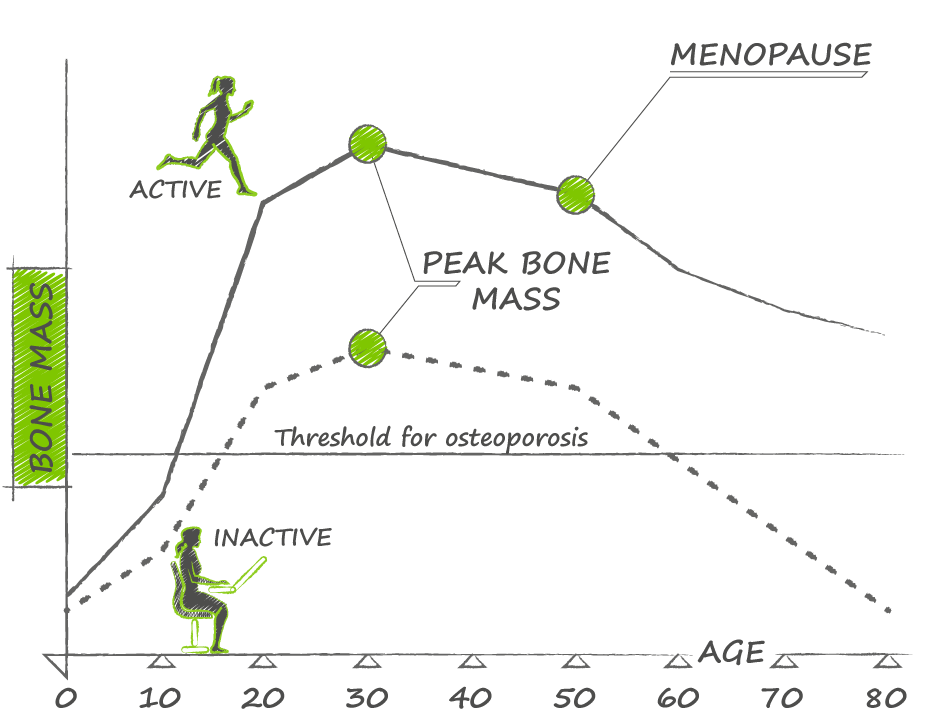 For women, the dramatic fall in estrogen levels (to 1% of pre-menopausal levels) is largely responsible for most of the bone loss, and replacement therapy is very effective at decreasing this rate of bone mass.
More importantly, estrogen replacement therapy has been definitively shown to decrease fractures. Estrogen replacement can reduce fractures from 33-50%. Most importantly this reduction also applies to hip fractures - recall that approximately 28% of women will die within 1 year of fracturing their hip. Estrogen replacement combined with exercise (which can also reduce risk of hip fracture by 38%) makes sense for any woman at high risk of osteoporosis. Of course a recommendation of estrogen replacement comes with some important considerations:
You may be interested: Reconsidering Estrogen Osteoporosis The Science of Bone Health - 3 Principles to Develop and Maintain Bone |
AuthorDr. Brendan Byrne Categories
All
|
 RSS Feed
RSS Feed