|
Last week, we covered a lot of ground and got very technical. The etiology of atherosclerosis, the disease process underlying heart disease and stroke - the #1 cause of death and disability in Canada. There were a number of takeaways that are worth reiterating:
This week we will get very practical and provide a framework for understanding risk and treating, preventing or reversing atherosclerosis. The first objective is to understand your risk. Since atherosclerosis is a process involving:
The challenge is that we do not have perfect metrics, with enough evidence in relation to the hard outcomes of cardiac events to be definitive. Here we can rely on some evidence-based risk calculators, like Framingham, that are based on large datasets. These generally are a good place to start:
In my practice - I start with Framingham, but also try and gather more data to support my understanding of the three ingredients: Endothelial dysfunction - the biggest factors to consider are
Oxidized LDL:
Inflammation:
Testing allows us to understand risk at a personal level, from here, my objective is to align my patient’s behavior with optimizing and reducing the risk across the three dimensions of atherosclerosis causality. The first place to start is with weight management - bringing the patient to normal levels of BMI, body fat and most importantly visceral fat will improve blood pressure, decrease insulin resistance, improve endothelial function, improve lipoproteins by increasing HDL-C and decreasing LDL-p, and decrease inflammation. For weight management - we nutrition comes first. Whole foods, mostly plant-based. We adjust and refine depending on response on our key biomarkers. Next we increase exercise. Our first goal is to get people to 150 minutes of moderate to vigorous exercise. Nothing magic here - there is ample evidence to support this level of exercise as the minimal effective dose. We adjust exercise across three components - aerobic, functional movement and resistance training. Again we adjust and refine depending on response of the patient’s biomarkers. Inadequate sleep and chronic stress have both been shown to affect inflammation, immune response and endothelial function - so we need to have a strategy to get at least 7 hours of high quality sleep and reduce stress. At Wellness Garage - we create month personalized lifestyle behavior action plans that we call “Precision Health Tune-ups”. We reassess every 4 months, until we have optimized behavior and reduced risk. If we see a patient’s measures of endothelial function, LDL and inflammation come to optimal levels with lifestyle measures we feel very comfortable that we have reduced their risk. When risk remains, we are comfortable with using both specific supplements and drug therapies to normalize BP, address LDL-p and other key biomarkers - there is, we believe, enough evidence to support this approach. In every case - this is a personal risk reduction conversation. Drug treatments are used to lower the probability of clinical atherosclerosis and carry a risk of adverse drug reactions. How much risk is too much on either side (disease vs drug reaction) of this decision is very individual - and can only be decided by a very well informed patient. In summary, atherosclerosis is a systemic, almost ubiquitous disease process with three major causal dimensions.
The place to start is with a medical assessment that measures at a minimum the key biomarkers for each dimension. Know your numbers. With this baseline, you will have an understanding of how your genes and current behaviors are working for you. The next step is to optimize your behaviors - nutrition, exercise, sleep, stress tolerance all play a role. After several months of modified behaviors, checking to see your body’s response allows you to optimize your behaviors and reduce risk. If, despite optimal behavior change, your risk does not seem to come down - supplements and medications may help. This is something that you need to work through with your physician. At Wellness Garage - we take a precision health approach to atherosclerosis prevention, treatment and reversal, by working with our members throughout this process - Assess, Change Behaviors, Re-assess and Adjust. If you would like our help to take control of your health please books free consultation.  This is the first of a two part series on atherosclerosis and will explain:
What is atherosclerosis? Atherosclerosis - commonly known as “ hardening of the arteries” refers to a disease process that causes damage to the arteries resulting in narrowing, blockage, occlusion and even rupture. Atherosclerosis is the underlying cause of most cardiovascular disease (CVD) - including heart disease and stroke.
Atherosclerosis is both very common and very preventable. Our view is that the key to prevention comes from really understanding how atherosclerosis develops. This involves getting past some common misconceptions that have resulted from an oversimplification of the disease through the two dominant conceptual models used to explain atherosclerosis:
The issue with each of these models is that they overlook some key facts and observations:
Before we go further here - let's back up and better understand the disease process:
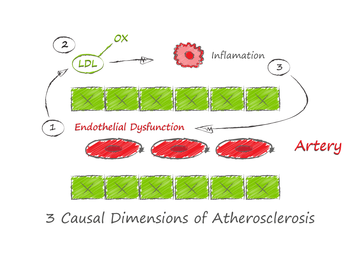
To summarize, atherosclerosis is caused by an inflammatory response to oxidized lipoproteins within the artery wall. There are three main ingredients that trigger a lesion:
The developing process can be mitigated in its earliest phases by HDL-particles that take away the sub-endothelial cholesterol - even after it is taken up by the foam cells. Evidence shows that the risk of atherosclerosis increases with increasing concentrations of LDL-particles in linear fashion - note this LDL-particle numbers, not LDL-cholesterol concentration. (while LDL-C and LDL-p are generally concordant, ie. they increase and decrease together, this is not always true - especially when insulin resistance is present). LDL-cholesterol is what is commonly reported on the standard lipid panel. A better test to understand your risk is the ApoB100 protein- which gives you the number of LDL-particles as each LDL-particle has one ApoB100 It must be stressed that LDL-P easily enter and exit the sub-endothelial space all the time - it is the oxidation of LDL-P that is key step in initiating atherosclerosis. Only oxidized LDP-P is taken up by macrophages and foam cells. What triggers the oxidation of the LDP-P? Damaged, inflamed or dysfunctional endothelial cells create the conditions for LDL-P oxidation. Common causes of endothelial dysfunction are:
Another key point is that the process that leads to an atherosclerotic lesion is systemic - so just identifying and treating lesions that cause blockage (ie. plumbing model) does not sufficiently decrease risk as there may be other non-obstructive lesions that can rupture and cause acute occlusion. So in essence, with atherosclerosis we have a reinforcing cycle of:
The take-home points to remember are:
At Wellness Garage - we can help you understand and take control of your health. Our comprehensive medical, fitness, nutritional and behavioral assessments give you baseline from which to measure your progress. Our coaching helps you improve your behaviors, one habit at a time. For more information - please book a free consultation. |
AuthorDr. Brendan Byrne Categories
All
|
 RSS Feed
RSS Feed