|
For many physicians of my era (started practice in 1991) the story of hormone replacement therapy reflects the bandwagon nature of medicine. In the mid-nineties as I opened my practice, we actively recommended that almost all menopausal women should take hormone replacement (HRT) or estrogen replacement therapy (if they had a hysterectomy). As physicians we measured ourselves by our HRT percentage - feeling that if we were doing our jobs this should approach 100%.  The reasons for our enthusiasm for estrogen replacement seemed clear. In menopause, estrogen levels plummet to 1% of pre-menopausal levels. Using estrogen to replace this loss, appeared to have significant benefits:
...and while these benefits were offset by a small but real increased risk in venous blood clots - the benefits seemed overwhelming. Then on July 17, 2002 the world of estrogen replacement came crashing down. The Woman's Health Initiative - the largest and most expensive trial ($1B) ever done at that time was stopped because HRT increased the risk of breast cancer by 26%. Overnight, physicians jumped off the bandwagon and rates of HRT fell dramatically. Unfortunately most of us did not read the details of the study (once it was eventually released).  In the new book, "Estrogen Matters" by Dr. Avrum Bluming and Carol Tavris, the data from WHI is examined in the broader context.
Starting with the conclusion that HRT increases breast cancer by 26% - the first and most stunningly underappreciated fact was that this increase did not meet statistical significance, meaning that it did not clear the commonly accepted threshold that there has to be less than a 5% chance that this result could be random. Next, even if you accepted that the result was real and not random, then it is important to understand the result. There are two ways that the study could have shown an increased rate of breast CA, either the rate of breast CA actually increased in the treatment group OR the rate of breast CA went down in the control group. Of course if the latter explanation is correct then the study is flawed. Closer analysis of the WHI data has clearly shown that the reported increase rate of breast CA did not come from higher breast cancer rates than expected in the treatment group but resulted from the fact that the control group had a lower incidence of breast cancer than expected. Even more confusing was the fact that this reduction of breast cancer in the control group occurred because there was a significant number of woman who had been on HRT previously and in this group there was less breast cancer. So the WHI concluded that HRT increases breast CA because previous HRT experience decreased the rate of breast CA in the control group - incredible! The third thing to consider when reviewing the WHI findings is the absolute rate of the increase in breast cancer. So even if you accept that the effect is real and not the result of randomness or a decreased rate in the control group the absolute increase in was 8 more breast cancer diagnoses per 10,000 patient years. Taken together, this review significantly decreases, if not removes altogether, the concern that I have about estrogen causing an increase in breast cancer. Bluming and Tavris then revisit the benefits and risks of HRT - providing links to the best available current evidence and in doing so provide perhaps the best single source of HRT information for anyone considering HRT. Summary of the Risks and Benefits of Estrogen Replacement: Benefits
Risks
Bottom Line: For every woman going through menopause, HRT should be given personalized and individualized consideration. I highly recommend this book to anyone who wants to review the data for themselves and make a fully informed decision. As for my physician colleagues, I have already been recommending "Estrogen Matters" For a great listen - check out Peter Attia's podcast. with Bluming and Tavris You may be interested: Osteoporosis Considering the Role of Estrogen Therapy Osteoporosis The Science of Bone Health - 3 Principles to Develop and Maintain Bone In our third bone health post we are going to look specifically at the medical approaches to supplement our lifestyle approach. Our conclusions will not change: The best osteoporosis strategy is to do everything to avoid the likelihood of falling, while providing the best lifestyle support to decrease the rate of bone loss. When it comes to osteoporosis, the strategy must be to decrease the consequences:
It is important to remember that there are more fractures in people who do not have osteoporosis than in people that do; again reiterating the point that preventing the falls that cause the fractures is the most important thing you can do to decrease risk. For woman at risk for osteoporosis, there is an additional strategy that must be considered - estrogen. The key risk factors for osteoporosis are:
For maintaining bone mass there is no other therapy as effective as estrogen replacement starting early in menopause. For both women and men - peak bone mass is achieved in early adulthood, and through an active lifestyle, with adequate nutrition (calcium and protein), and Vitamin D, maintained until middle age when it begins to drop more rapidly. 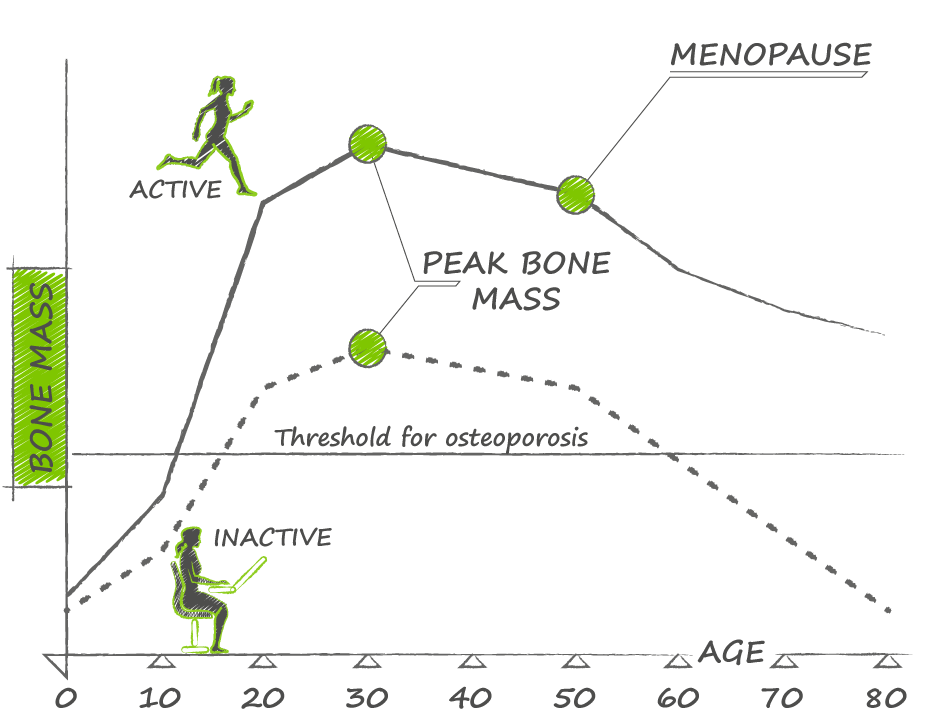 For women, the dramatic fall in estrogen levels (to 1% of pre-menopausal levels) is largely responsible for most of the bone loss, and replacement therapy is very effective at decreasing this rate of bone mass.
More importantly, estrogen replacement therapy has been definitively shown to decrease fractures. Estrogen replacement can reduce fractures from 33-50%. Most importantly this reduction also applies to hip fractures - recall that approximately 28% of women will die within 1 year of fracturing their hip. Estrogen replacement combined with exercise (which can also reduce risk of hip fracture by 38%) makes sense for any woman at high risk of osteoporosis. Of course a recommendation of estrogen replacement comes with some important considerations:
You may be interested: Reconsidering Estrogen Osteoporosis The Science of Bone Health - 3 Principles to Develop and Maintain Bone Osteoporosis is “a skeletal disorder characterized by compromised bone strength, predisposing to an increased risk of fracture” (Osteoporosis 2000). One in three women and one in two men will suffer an osteoporotic fracture in their lifetime. 80% of all fractures in people over the age of 50 are a consequence of osteoporosis. Of the various osteoporotic fractures, hip fractures are the most devastating:
Unfortunately, all too often, a fracture is the first indication that a person is affected by osteoporosis. 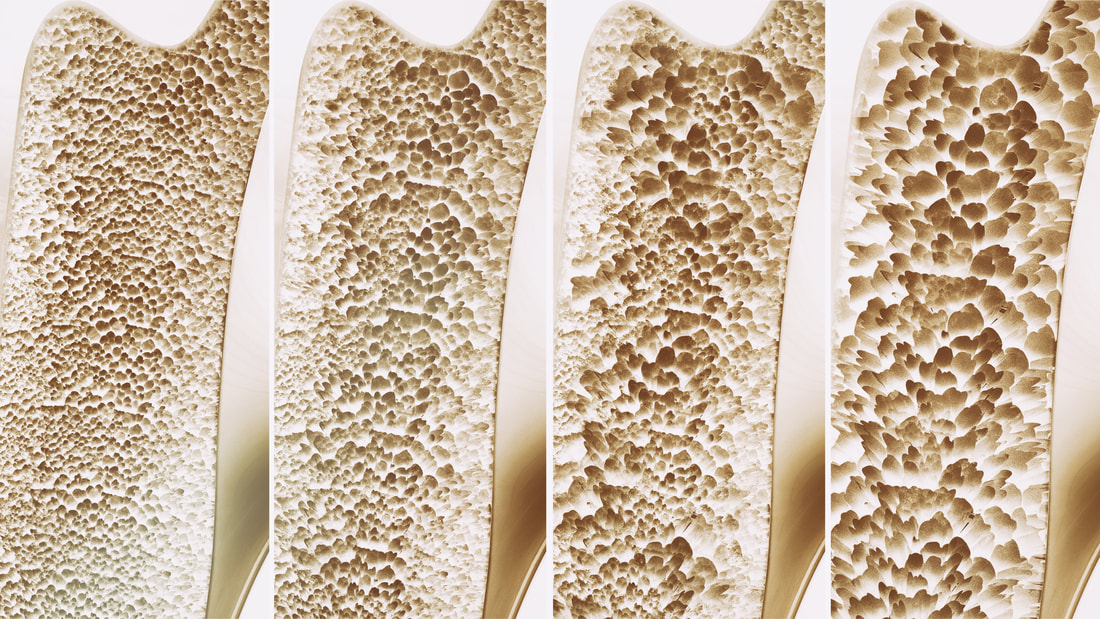 To understand why osteoporosis happens and to develop a strategy to prevent its consequences, we must understand how bone works. Last week we reviewed the dual, competing functions of bone: Bone acts as structure as well as reservoir for calcium and phosphorus act in competition. Bones must be strong and flexible to respond to the weight bearing and mechanical forces of our activities. When our activities increase in intensity, our bones get stronger in order to sustain the load. However if calcium or phosphorus are in short supply, our regulatory hormones will draw them out of bone to serve vital function in other cells in the body, and in the process potentially weaken bone. Bone is an incredible material providing both strength and flexibility in order to be resilient to the mechanical forces imposed by daily activities. To accomplish this bone is a composite material made of minerals bound to protein, predominantly collagen. If bone was made only from mineral crystals it would be brittle and fracture easily; if made solely from protein it would be too flexible and would not provide adequate structure and flexibility. Bone is also a dynamic material always changing and growing, responding to mechanical loads, resorbing and laying down new bone through the balanced effects of osteoclasts and osteoblasts. During our childhood, as our bones are growing both cell types are constantly working, osteoclasts reshaping and osteoblasts rebuilding bone with osteoblast activity predominanting so that bone length, thickness and overall mass increase as our bodies grow in stature. Once growth is finished and we are adults, osteoblasts spend less time creating new bone and more time regulating bone repair - osteoblasts signal osteoclasts to hollow out bone in a specific location and then fill in that area with new & healthy bone. To build and maintain our bones three general principles emerge:
Osteoporosis has been described as a pediatric disease with geriatric consequences, because our bone mass peaks when we are young (16-20 in women, and 20-25 in men). As young adults, our goal is to maintain bone density and strength through the three principles. But even with excellent bone habits, we all begin to lose bone in our mid 30's.  For woman the situation is more challenging as the precipitous drop in estrogen that occurs in menopause causes rapid bone loss, and is the reason why woman are more affected by osteoporosis than men.
So, the question for middle age to older people is how do the three principles work to avoid the consequences of osteoporosis? The key here is to think about more than bone density, to develop a strategy to decrease the consequences of osteoporosis: debilitating and life shortening fractures. Looked at from this angle - Principle 1 - use your bones to increase their strength is most important. Moderate to vigorous exercise is associated with a 45% and 38% reduction in hip fractures in men and women respectively. Exercise helps slow the loss of bone that comes with ageing in both men and women, but this is not how it decreases hip fracture risk. Exercise works by reducing the risk of falling in the first place. Developing an exercise strategy that focuses on maintaining strength, functional movement and balance is the best thing you can do to avoid the consequences of osteoporosis - regardless of bone density. What about Principle #2 - supplying your body with the key ingredients to develop bone? This is absolutely key in the bone developing years as teenagers and young adults, and likely important through middle age, but it is not sufficient to decrease fracture risk. A systematic review published in 2015 by Boland et. al concluded that "dietary calcium intake is not associated with risk of fracture, and there is no clinical trial evidence that increasing calcium intake from dietary sources prevents fractures. Evidence that calcium supplements prevent fractures is weak and inconsistent." Complicating matters further, there is some evidence that calcium supplements may be associated with cardiovascular risk though the evidence is inconsistent and inconclusive. Many clinicians have moved away from recommending calcium supplements, instead recommending that adequate calcium intake be achieved through nutrition. Given the high calcium content of green leafy veggies - this is definitely the position we take. As for Vitamin D, there are so many benefits of "D" beyond bone that the lack of clinical trial evidence to support a reduction in fracture reduction, does not change our view that maintaining optimal Vitamin D levels must be part of any strategy for long term health and vibrancy. Principle #3 - holds firm - while bone loss is inevitable with ageing - it is essential to avoid substances that accelerate bone loss. Bottom Line: When it comes to osteoporosis, the strategy must be to decrease the consequences:
Decreasing bone density is an inevitable part of ageing - our bone density peaks in our early years, is maintained up to middle age and declines thereafter. If we live long enough, our bones will become thinner. Whether they reach the diagnostic levels of osteoporosis is less important than our ability to avoid falling. The best osteoporosis strategy is to do everything to avoid the likelihood of falling, while providing the best lifestyle support to decrease the rate of bone loss. While this advice applies equally to men and women, we have left out something for women - the role of estrogen in bone loss and osteoporosis, and the risks and benefits of estrogen replacement as an osteoporosis strategy...more on this next week. You may be interested: Osteoporosis Considering the Role of Estrogen Therapy The Science of Bone Health - 3 Principles to Develop and Maintain Bone Our bones are remarkable examples of evolution's ingenuity. From a functional perspective, bones serve multiple roles - structure, mobility, support, protection as well as serving as a reservoir for essential minerals. These roles became important, when our distant predecessors left the calcium-rich ocean to live in calcium-poor fresh water, and then further evolved to live on land where gravitational forces (without the buoyancy effect of water) put greater stress on the skeleton. 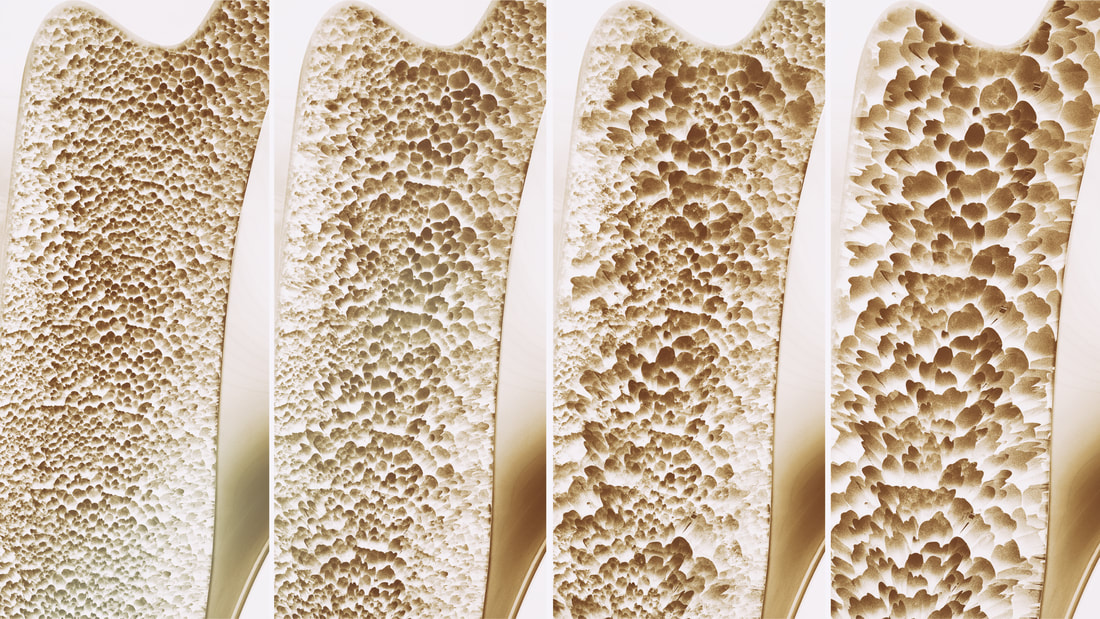 Our skeletons store two key minerals, calcium and phosphorus, both essential for the healthy functioning of cells and bodily organs, and our bones are called, in times of stress, to maintain blood levels of both.
A complex system of hormones regulates calcium and phosphorus in our bodies acting on bone, intestine and kidneys to maintain adequate supply for proper cellular function in all cells but particularly in nerves and muscle. These hormones include: Calcium Regulating Hormones
Of these, Vitamin D stands out, as we are dependent on our environment, specifically sunlight to synthesize adequate Vitamin D to maintain adequate dietary calcium absorption from our intestines. The dual roles of bone, to act as structure and at the same time represent a reservoir for calcium and phosphorus, are in direct conflict with each other. Bones must be strong and flexible to respond to the weight bearing and mechanical forces of our activities. When our activities increase in intensity, our bones get stronger in order to sustain the load. However if calcium or phosphorus are in short supply, our regulatory hormones will draw them out of bone to serve vital functions in other cells in the body, and in the process potentially weaken bone. Bone is an incredible material providing both strength and flexibility in order to be resilient to the mechanical forces imposed by daily activities, not to mention sports. To accomplish this bone is a composite material made of minerals bound to protein, predominantly collagen. If bone was made only from mineral crystals it would be brittle and fracture easily; if made solely from protein it would be too flexible and would not provide adequate structure and flexibility. The mineral components of bone are crystals of calcium and phosphate called hydroxyapatite. They are bound in a matrix to a triplet of three long, thin, intertwined collagen rods with are strengthened by chemical bonds between proteins. Other proteins further strengthen the collagen matrix and regulate mineral binding. Small changes in shape of the bones, from mechanical forces, act on the cells inside the bone to send signals that allow bone to respond to these loads by remodelling and strengthening. In this way, our bones are always changing and growing, responding to mechanical loads, resorbing and laying down new bone. Bone health depends on the balanced effects of two kinds of bone cells:
Once growth is finished and we are adults, osteoblasts spend less time creating new bone and more time regulating bone repair - osteoblasts signal osteoclast to hollow out bone in a specific location and then fill in that area with new & healthy bone. Bone also has another remarkable feature - it is anti-fragile: if stressed it gets stronger. This phenomena, called Wolff's Law was originally recognized in late 19th century, but is probably most dramatically visualized in tennis players who show far greater bone mass in their racket arm as compared to their non-dominant arm. This remarkable gift, that our bones grow stronger through stress and usage has a dark, flip side: our bones grow weaker through disuse. Only in modern times has this become a downside. For most of human history, our lives were simply too active. Our predecessors had very strong bones from all the physical work and stress placed on their bones throughout their lives. From the industrial revolution on onward, labor saving technologies have decreased the degree to which we need to use our bodies to the point that many of us are no longer building enough bone. This is another example of evolutionary mismatch that I have previously written about. Compounding this fundamental mismatch, modern diets and lifestyles also lead to deficiencies in dietary calcium, protein and Vitamin D necessary for bone health. To develop and maintain bone mass three key principles emerge:
Next week, we will look at osteoporosis and what you can do to prevent or reverse it. |
AuthorDr. Brendan Byrne Categories
All
|
 RSS Feed
RSS Feed